“Designer” Corneal Surgery
Corneal transplantation is the most common transplant surgery worldwide, and it has come a long way. Dr. Guillermo Rocha explains how recent innovations are improving safety, speeding recovery, and helping patients regain clearer vision.

Dr. Guillermo Rocha
Chair, Department of Ophthalmology & Visual Sciences, McGill University
Physician-in-chief, Ophthalmology McGill University Health Centre (MUHC)
Montreal, QC
Understanding corneal transplant surgery
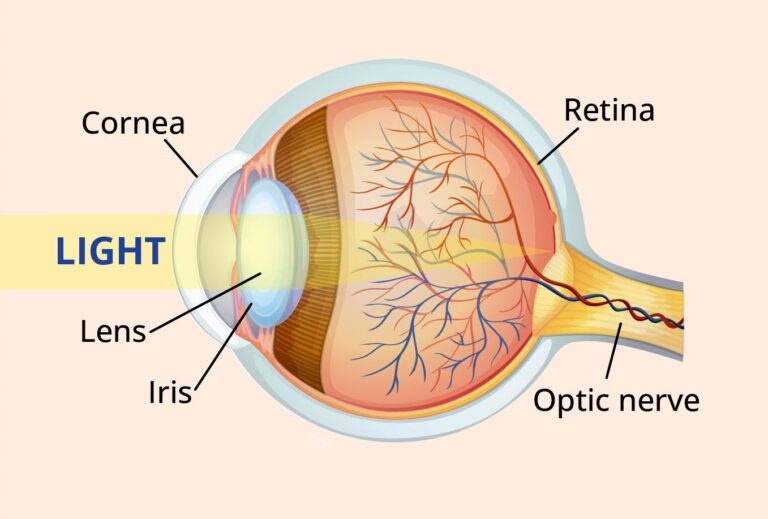
The cornea is the clear, dome-shaped portion at the front of the eye. It helps focus light, bending it toward the lens and retina. In fact, the cornea is responsible for about 70% of the eye’s focusing power.
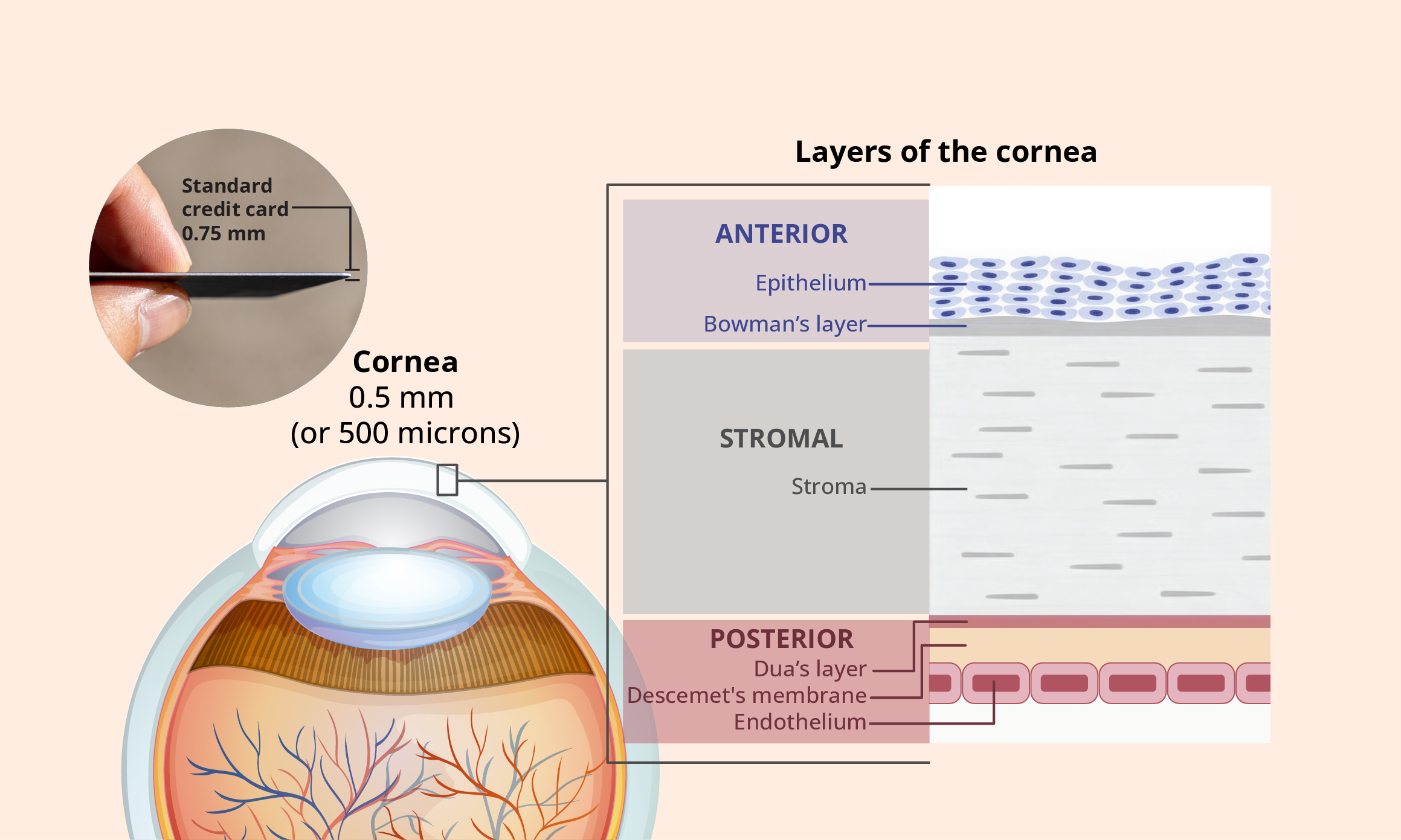
The cornea is incredibly thin. At only half a millimeter thick, it’s thinner than a credit card! Despite this delicate structure, the cornea is made up of several distinct, specialized layers.
How corneal transplant surgery has evolved
1905
First successful
corneal
transplant
Dr. Eduard Zirm performed the first successful corneal transplant on a farm worker with damage to both corneas caused by chemical burns. The procedure was a full-thickness transplant, known as a penetrating keratoplasty, in which the entire cornea is replaced.
20th Century
Steady surgical advances
Advances in donor eye banking, operating microscopes, and surgical tools improved the safety and success of corneal transplants. For decades, full-thickness transplantation remained the standard
surgical technique.
Early 2000s
The partial-
thickness
transplant
revolution
Surgeons started using layer-specific techniques that replace only the damaged parts of the cornea, improving recovery and outcomes.
The era of “designer” corneal surgery: treating only what’s needed
Today, corneal surgery is no longer one-size-fits-all. Rather than replacing entire cornea, we can now tailor surgery to each patient’s specific needs. Using OCT and other imaging tools, we can create a 3D map of the surface and thickness of the cornea and identify damaged or disease areas down to the micron level. This allows us to plan highly customized, topography- and tomography-guided surgery with remarkable precision.
“The key is that we’re customizing surgery to the patient. We’re no longer replacing the whole cornea, but targeting different layers. In many cases, only the affected layers of the cornea are replaced, preserving as much healthy tissue as possible.”
– Dr. Rocha
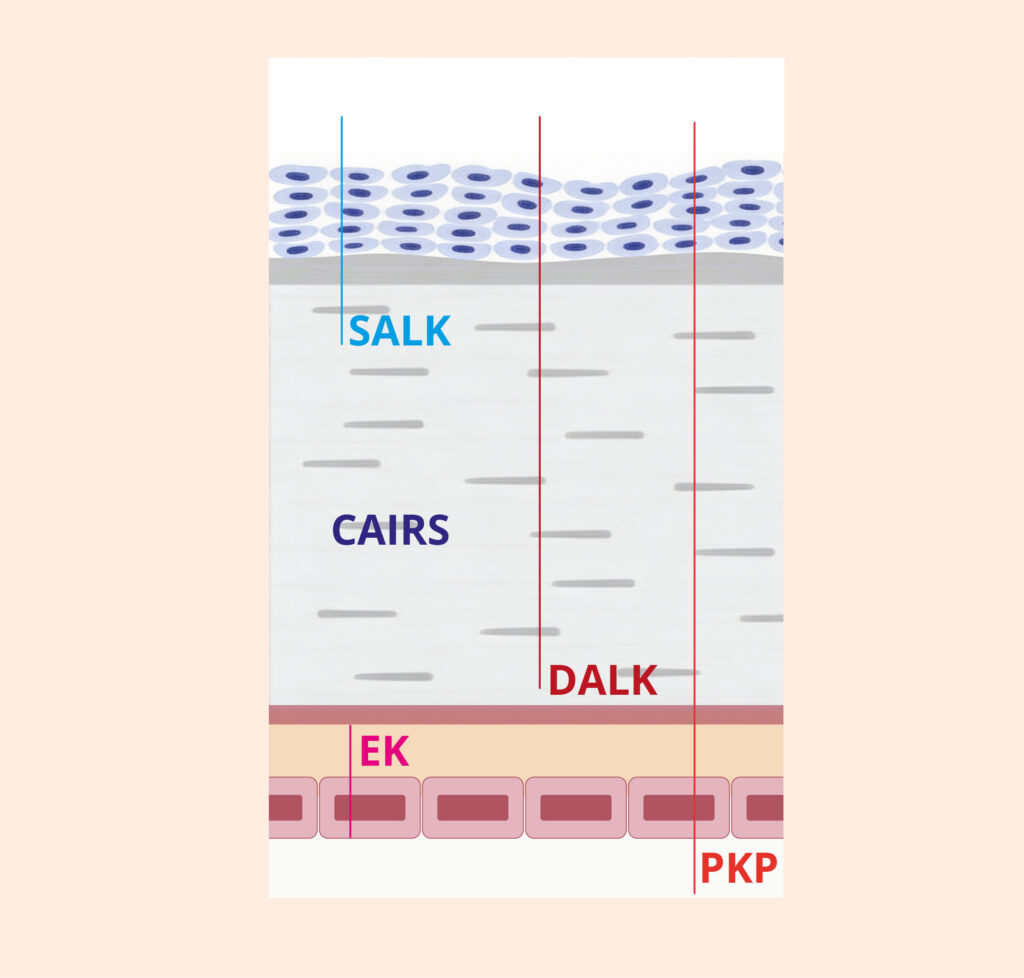
Modern procedures are designed to treat different layers of the cornea, depending on where the problem lies:
- A full-thickness transplant
- Replaces the entire cornea with healthy donor tissue
- Still used when all layers of the cornea are affected
- Replaces only the outer surface layers of the cornea
- Used for shallow scars or surface disease
- Replaces the front and middle layers; the back layer (endothelium) is kept intact
- Commonly used to treat keratoconus (a condition where the cornea thins and bulges into a cone shape)
- Tissue segments from the donor cornea are made and inserted into the patient’s cornea
- Reshapes the cornea without a full transplant
- Used for keratoconus
- Replaces only the back cell layers of the cornea through a small incision; most of the cornea is left intact
- Common procedures are Descemet’s Membrane Endothelial Keratoplasty (DMEK) and Descemet’s Stripping Automated Endothelial Keratoplasty (DSAEK), which differ in the thickness of the graft used
- Used if the endothelium fails (due to inherited conditions or complications from previous surgeries)
Femtosecond lasers: transforming corneal surgery

One of the most important recent innovations in corneal surgery is the use of femtosecond lasers. These ultrafast, bladeless lasers allow us to create highly precise, microscopic cuts in the cornea. Compared to traditional manual techniques this leads to better accuracy, improved wound healing, and faster recovery.
Canada has been at the forefront of using femtosecond laser for therapeutic corneal surgery. In March 2026, McGill University Health Centre unveiled a new femtosecond laser at Lachine Hospital in Montreal, recognized as the most advanced system for corneal surgery. As the first of its kind in a Canadian public hospital, it expands access and enables more personalized treatment for patients.


What this means for patients
For patients, these advances have transformed the
experience of corneal transplant surgery.
Compared to traditional, full-thickness transplants, today’s tailored approaches offer:
• Less invasive care
• Lower risk of complications and tissue rejection
• More precise, targeted treatment
• Faster recovery
• Better quality of vision
The result is better outcomes and better quality of life for our patients.
“The biggest change we’ve seen is how much easier the experience can be for patients. With newer, less invasive approaches, recovery is faster, the risks are lower, and the quality of vision is often better. And as these techniques continue to evolve, we expect outcomes to keep improving even further.”
– Dr. Rocha