Eye injuries are common and can cause anything from minor scratches to the cornea to vision loss or even blindness. Even if you think an injury is minor or are unsure you have an eye injury, it’s best to get checked out by your eye doctor. In general, anything other than small scratches or grit in the eye may be potentially serious.
Signs of a potentially serious eye injury are:
Continuous eye pain
Difficulty seeing
One eye not moving as well as the other
Cut/torn eyelid
One eye sticking further out of its socket
Unusual pupil size or shape
Something in the eye that can’t be removed by tears/blinking
Blood in the clear part of the eye (the clear, dome-shaped area at the front of the eye between your cornea and iris)
Causes
Common causes of eye injuries are:
Blows to the eye (e.g., from balls or hands)
Pieces of flying debris from explosions or industrial work
Darts, fireworks, bullets
Chemical splashes
Risk Factors
You may be more at risk of getting any eye injury if you:
Play a sport, particularly a contact sport
Work in construction or an industrial setting
Work around chemicals
Don’t use protective eyewear
Diagnosis
What happened to your eye will determine what tests a doctor uses to make a diagnosis. First, your doctor will need to know exactly what happened to your eye. This will help him or her decide what diagnostic tests to use.
Below are some of the tests an eye doctor may use to make a diagnosis of an eye injury.
Visual acuity test
This test helps your eye doctor see if you’ve had any changes in your vision. You’ll be asked to look at an eye chart with different sizes of letters on it. Your doctor will test one eye at a time, with the other eye covered.
Slit-lamp examination
A slit lamp allows your eye doctor to view different parts of your eye up close to see if there are any problems. This device is called a “slit lamp” because it uses a bright line of light to illuminate the different parts of your eye.
Retinal exam
Your doctor will perform a retinal exam to look for damage in the back part of the eye. Eye drops will be placed into the eyes to widen the pupils. Your doctor will then use a device called an ophthalmoscope to get a good look at your retina.
Fluorescein eye stain test
This test is used to see if you have any scratches on your cornea. Your eye doctor will put drops of a dark orange dye called fluorescein in your affected eye. He or she will then shine a special blue light into your eye. Any areas that are damaged will appear green.
X-ray
In some cases, your doctor may order an X-ray. This will help him or her to see if you have a fracture in your eye bone, or if there are any foreign objects inside your eye.
Ultrasound
If your eye doctor cannot see into the back of the eye, he or she may also order an ultrasound. This test uses high-frequency sound waves to create a picture of structures in the back of the eye.
Treatment
How your eye injury is treated depends on what the injury is and how severe it is. Below are some general guidelines.
Eye Scratches & Corneal Abrasions
Most eye scratches and corneal abrasions are minor and will heal on their own within a few days to a week. Still, if you’ve scratched your eye, it’s a good idea to see your eye doctor. If you’re in a lot of pain or are having difficulty seeing, it is important to have the eye assessed quickly.
Treatments you may be prescribed by your eye doctor include: • Antibiotic eye drops or ointment to treat infection • Steroid eye drops to treat inflammation • Eye drops to lubricate your eyes.
Small Particles in the Eye
Our eyes are good at flushing natural particles like sand or dirt out through tears and blinking. This is usually not an emergency. Man-made particles like metal or glass, however, may be cause for concern. These kinds of particles can stick in the eye and create lasting irritation.
Whatever the particle, if you continue to feel like there’s something in your eye, see your eye doctor or go to your nearest emergency room.
General tips for dealing with particles in your eye:
Do notrub your eye
Try to allow your natural tears to flush out the particle; try blinking several times
Use saline solution or tap water to flush out your eye
Getting Hit in the Eye
If you have a black eye or notice any pain or changes in your vision ‑ even after a slight blow ‑ see your eye doctor or visit the emergency room.
General tips for managing a blow to your eye:
Do notput any pressure on your eye
Apply a cold compress GENTLY to help reduce pain and swelling
Eye Cut or Puncture
If your eye has been cut or punctured, see your eye doctor or get medical attention right away.
Carefully place a protective shield over the eye (e.g., bottom of a paper cup taped to the skin around your eye); be careful not to press the shield directly against the eye.
DO NOTdo any of the following:
Rub your eye or apply pressure to it
Rinse your eye with water
Try to remove any objects that are in your eye
Take aspirin, ibuprofen, naproxen or other non-steroidal anti-inflammatory medications as these may cause you to bleed more
Splashes/Chemical Burns in the Eye
If any chemicals get splashed in your eye or you suffer a chemical burn in your eye, follow these steps:
Immediately flush your eye with lots of clean water
Get emergency medical help right away
Try to find out the name of the chemical—this will help the doctor know how to treat your eye
If you have diabetes mellitus, your body does not use and store glucose properly.
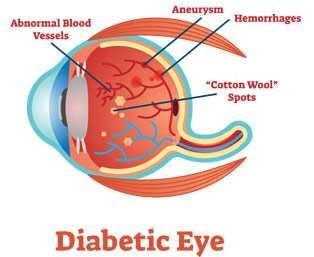
Over time, diabetes can damage blood vessels in the retina (the inner layer of tissue that lines the back of the eye). The retina is composed of a network of nerves that sense light and help to send images to the brain.
The damage to retinal blood vessels is referred to as diabetic retinopathy.
The various stages or types of diabetic retinopathy include:
Nonproliferative diabetic retinopathy (NPDR)
In this early stage, tiny blood vessels within the retina leak blood or fluid causing the retina to swell or to form deposits called exudates. Many people with diabetes have mild NPDR that does not affect their vision.
Macular edema
Refers to the swelling or thickening of the macula (the centre of the retina that allows us to see find details clearly) caused by fluid leaking from the retinal blood vessels. This is the most common cause of visual loss in diabetes. Vision loss may be mild to severe, but in the worse cases side vision can continue to function.
Macular ischemia
Refers to the closing of capillaries (or small blood vessels) in the retina. Vision blurs because the macula no longer receives sufficient blood supply to work properly.
Proliferative diabetic retinopathy
Refers to the growth of abnormal blood vessels from the surface of the retina inwards into the vitreous cavity. These vessels are fragile and can break and bleed, obstructing vision or they can produce scar tissue that distorts the retina or in extreme cases causes it to detach from the wall of the eye. These vessels develop as a result of closure of the normal blood vessels in the periphery of the retina as a result of diabetic damage.
Causes
Diabetic retinopathy can arise when you have diabetes mellitus.
If you have diabetes mellitus, your body does not use and store glucose properly.
Over time, diabetes can damage blood vessels in the retina (the inner layer of tissue that lines the back of the eye). The retina is composed of a network of nerves that senses light and helps to send images to the brain.
Risk Factors
If you have diabetes, early detection of diabetic retinopathy is the best protection against loss of vision.
You can significantly lower your risk of vision loss by maintaining strict control of your blood glucose and visiting your ophthalmologist regularly.
People with diabetes should schedule examinations at least once a year.
Pregnant women with diabetes should schedule an appointment in their first trimester, because retinopathy can progress quickly during pregnancy.
Diagnosis
People with diabetic retinopathy may have few symptoms until it is very advanced and difficult to treat.
To prevent progression of diabetic retinopathy, people with diabetes should control their levels of blood sugar, blood pressure and cholesterol. There is considerable evidence to suggest that rigorous control of blood sugar decreases the chance of developing serious proliferative diabetic retinopathy.
A medical eye examination is the only way to discover any changes inside your eye.
If the eye examination finds diabetic retinopathy, you may require a special test called fluorescein angiography or optical coherence tomography (OCT) to find out if you need treatment.
More frequent medical eye examinations may be necessary after a diagnosis of diabetic retinopathy.
Treatment
During the first stages of diabetic retinopathy, no treatment is needed, unless you have macular edema.
Once you have advanced stages of diabetic retinopathy, there may be certain treatments to improve your vision.
These drugs are the first line of treatment for diabetic macular edema and are injected into the eye regularly to reduce leakage and improve vision (see also AMD for more information on how these work).
Focal laser treatment
This procedure is less commonly used now that anti-VEGF drugs are available.
Macular ischemia
Unfortunately, there are currently no effective treatment options available.
Proliferative diabetic retinopathy
Pan-retinal photocoagulation
This laser surgery may be used to shrink the new, fragile, abnormal blood vessels and reduce the risk of bleeding. During two or more treatment sessions, your doctor places laser burns in the areas of the retina away from the macula, causing the abnormal blood vessels to shrink. While there may be some loss of side vision and night vision, this procedure can prevent severe vision loss.
Vitrectomy
If the bleeding in your eye is severe and does not clear within a reasonable time, or if a retinal detachment is detected, an operation called a vitrectomy can be performed. During a vitrectomy, a retinal specialist removes the hemorrhage and any scar tissue that has developed, and performs laser treatment to prevent new abnormal vessel growth.
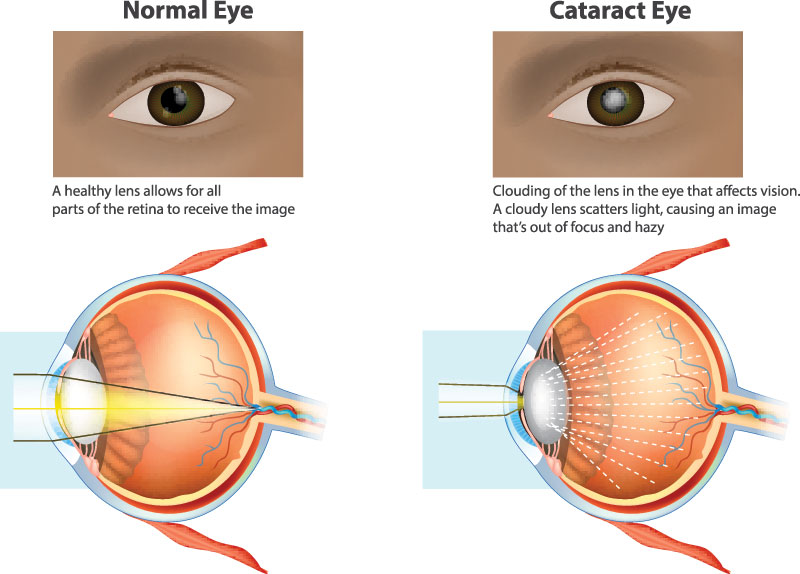
Your eye works a lot like a camera. Light rays focus through your lens onto the retina, a layer of light-sensitive cells at the back of the eye. Similar to photographic film, the retina allows an image to be “seen” by the brain.
Over time, the lens of your eye can become cloudy when normal proteins in the lens begin to break down. This prevents light rays from passing clearly through the lens. When the lens becomes cloudy enough to obstruct vision to a large degree, it’s called a cataract.
Cataracts can cause cloudy vision.
Cataracts usually develop slowly, causing a gradual and painless decrease in vision. Changes you might experience include:
Blurry vision
Glare, particularly at night
Frequent changes in your eyeglass prescription
A decrease in colour intensity
A yellowing of images
Improved close-up vision for farsighted (presbyopic) people
Reduced distance vision for nearsighted (myopic) people
The loss of transparency may be so mild that vision is barely affected, or it can be so severe that no shapes or movements are seen – only light and dark.
Causes
The most common cause of cataract is aging. Normal changes to the eye start happening around the age of 40. People over the age of 60 usually start to experience some lens clouding. Occasionally, babies are born with a cataract.
Risk Factors
The following factors can lead to cataracts:
Being over the age of 60
Eye injury
Some medications (e.g., steroids)
Systemic diseases such as diabetes
Being a smoker
Spending a lot of time in the sun without sunglasses that protect your eyes from harmful ultraviolet (UV) rays
Having close family members that have cataracts
Reducing your exposure to ultraviolet light by wearing a wide-brimmed hat and sunglasses may reduce your risk for developing a cataract, but once one has developed, there is no cure except to have the cataract surgically removed.
Diagnosis
To see if you have cataracts, your eye doctor will ask you about your medical history and the symptoms you have. They will also perform an eye exam and conduct a few tests:
Visual acuity test
This test helps your eye doctor see if you’ve had any worsening in your vision. You’ll be asked to look at an eye chart with different sizes of letters on it. Your doctor will test one eye at a time, with the other eye covered.
Slit-lamp examination
A slit lamp allows your eye doctor to view different parts of your eye (cornea, iris and lens) up close to see if there are any problems. This device is called a “slit lamp” because it uses a bright line of light to illuminate the different parts of your eye.
Treatment
Eyeglasses
Eyeglasses or contact lenses can usually correct slight vision changes caused by early cataracts, but they cannot sharpen your vision if you have a severe cataract.
Cataract surgery
If a cataract is affecting your vision enough to interfere with your normal lifestyle, it may be time to consider cataract surgery. Your ophthalmologist can help you decide if surgery is the best option for you.
During this outpatient surgical procedure, an ophthalmologist removes the cataract by making a small opening in the cornea at the front of the eye. The cloudy lens is broken into small pieces and removed through an ultrasonically vibrating needle that acts as a miniature “jackhammer”. A synthetic intraocular lens (IOL) is inserted to replace the focusing power of the natural lens.
You can learn about the different types of lenses and which option may be right for you in our Cataract Surgery Guide.
Cataract surgery is a very successful operation. One and a half million people have this procedure every year in North America, and over 95% have a successful result.
Age-related macular degeneration (AMD) is one of the most common causes of poor vision after age 60. In fact, it accounts for 90% of new cases of legal blindness in Canada.
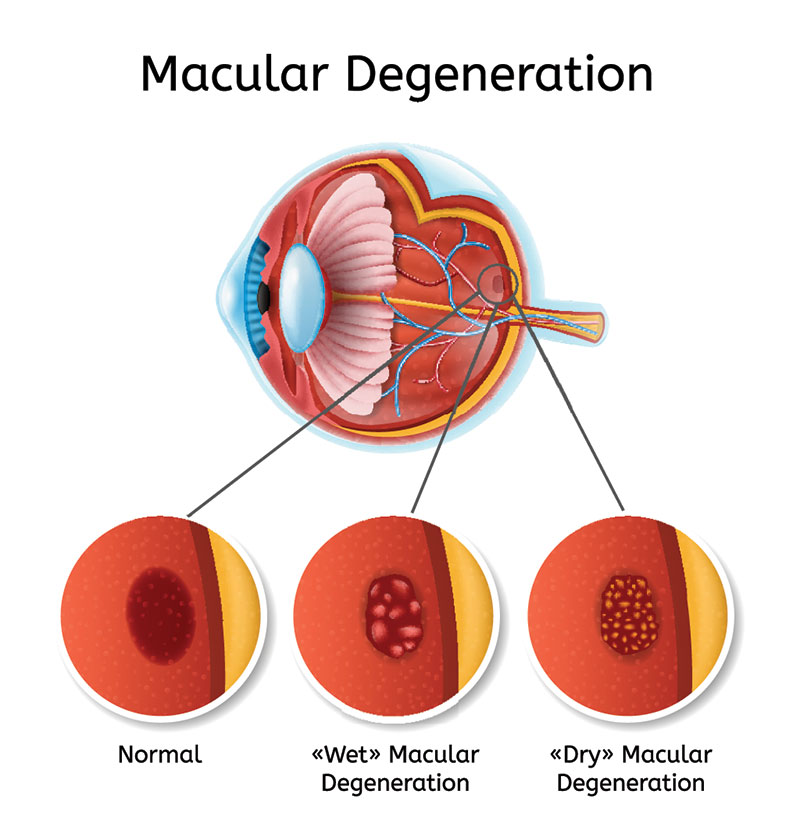
The macula is a small area at the centre of the retina in the back of the eye that allows us to see fine details clearly and perform activities such as reading and driving. AMD happens when the “seeing cells” in the macula break down or deteriorate.
The visual symptoms of AMD involve loss of central vision. While peripheral (side) vision is unaffected, with AMD, one loses the sharp, straight-ahead vision necessary for driving, reading, recognizing faces, and looking at detail.
There are two types of AMD: “dry” AMD and “wet” AMD.
Dry AMD
Nine out of 10 people who have AMD have atrophic or “dry” AMD. Dry AMD happens when the macula gets thinner and clumps of waste by-products accumulate beneath it. This causes you to slowly lose your central vision.
Wet AMD
Exudative or “wet” AMD is less common (affecting 1 out of 10 people with AMD) but is more serious.
In the wet form of AMD, abnormal blood vessels may grow in a layer beneath the retina. These vessels leak fluid and blood, scarring the macula. This causes a distortion and a large blind spot in the centre of your vision.
Promising AMD research is being done on many fronts. So far, research has resulted in the development of effective drugs to limit the damage from wet AMD and, in many cases, improve vision. Promising treatments for dry AMD are now entering clinical trials. In addition, high-intensity reading lamps, magnifiers and other low-vision aids help people with AMD to maximize their eyesight.
Causes
The causes of macular degeneration appear to be a mixture of genetics, aging and a mixture of other health and environmental factors.
Risk Factors
Age is the most significant risk factor for developing AMD, but you may be more likely to develop AMD if you:
Have blue eyes
Have high blood pressure
Have heart disease
Have high cholesterol
Smoke
Are overweight
Frequently eat foods high in saturated fat (e.g., butter, cheese)
Have a family history of AMD
Diagnosis
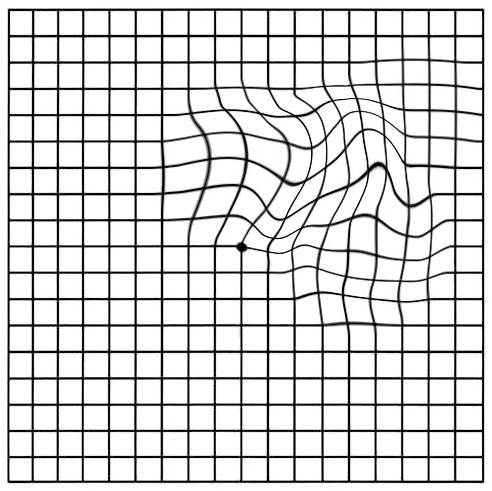
Early AMD changes can be detected at home with the use of an Amsler grid. Patients should test one eye at a time, covering the other eye and looking at the grid.
If the lines of the grid appear wavy, distorted or missing, the test is abnormal and the finding should be investigated by an optometrist or ophthalmologist.
Dry AMD usually progresses slowly over many years. Studies do NOT show that the rate of deterioration changes with the use of your eyes for reading and other pursuits. A specific vitamin regimen based on the AREDS (Age-Related Eye Disease Study) has been shown to reduce the rate of people with advanced dry macular degeneration developing wet AMD. Several promising drugs are undergoing clinical trials.
Wet AMD Treatments
Because the “wet” type of AMD can lead to vision loss quickly, treating wet AMD is time-sensitive. Delays can result in poorer outcomes. This is why people with AMD need to check vision in each eye regularly (see above) and report changes without undue delay.
Wet-AMD is most commonly treated through injections of anti-vascular endothelial growth factor (anti-VEGF) drugs directly into the eye. These drugs are very effective at causing the abnormal blood vessels to become dormant and stop growing and leaking. Unfortunately, the effect of currently available drugs wears off and they need to be injected regularly to prevent recurrence and vision loss. With treatment we expect up to 90% of eyes to stabilize. Up to a third of eyes improve.
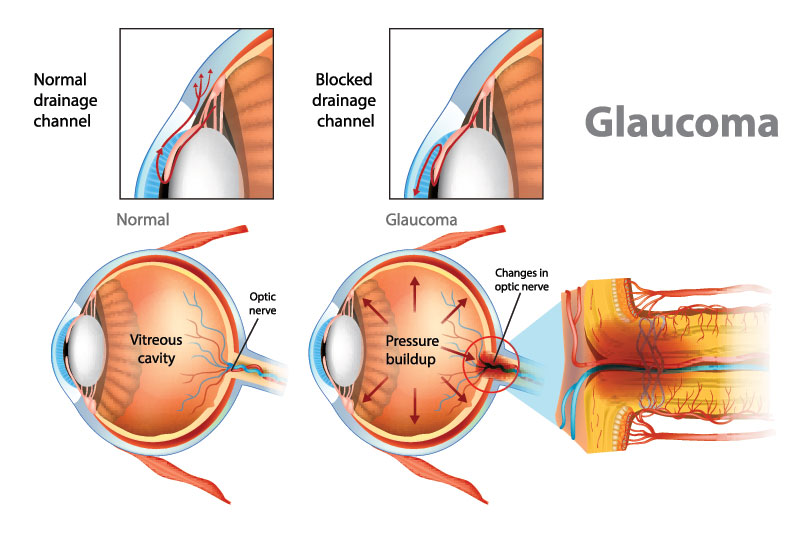
Glaucoma is a disease of the optic nerve. The optic nerve transmits the images you see from the eye to the brain and is made up of many nerve fibres (like an electric cable with its numerous wires).
Glaucoma damages nerve fibres, which can cause blind spots and vision loss.
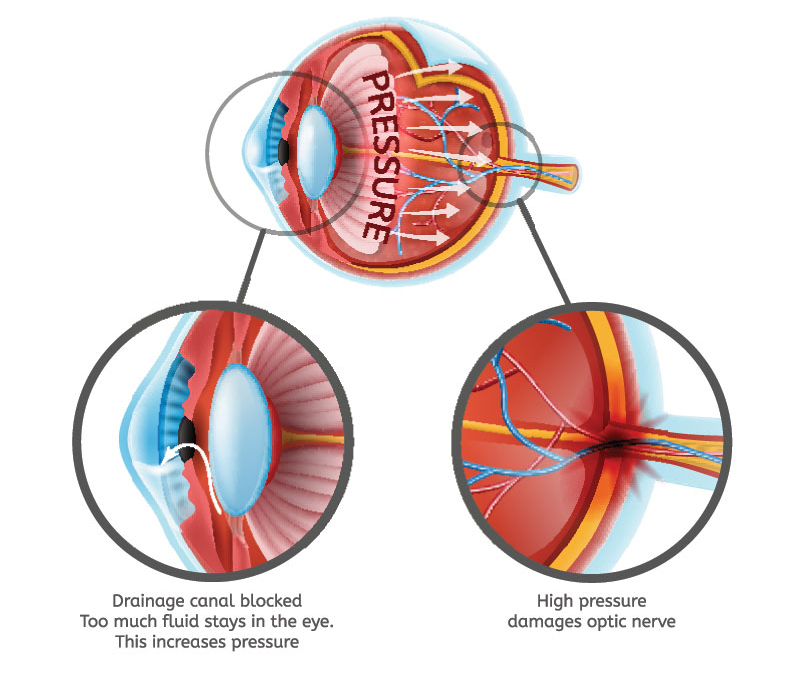
Glaucoma is usually related to the pressure inside the eye, known as the intraocular pressure (IOP). When the aqueous humour (a clear liquid that normally flows in and out of the eye) cannot drain properly, pressure builds up in the eye. The resulting increase in IOP can damage the optic nerve and lead to vision loss.
Causes
Open-angle glaucoma
The most common form of glaucoma is primary open-angle glaucoma. In this type of glaucoma, the aqueous fluid (thin, watery liquid in your eye) is blocked from flowing out of the eye at a normal rate through the tiny drainage system.
Most people who develop primary open-angle glaucoma notice no symptoms until their vision is impaired.
Ocular hypertension (or high internal eye pressure) is often a precursor to actual open-angle glaucoma. When ocular pressure is above normal, the risk of developing glaucoma increases.
Angle-closure glaucoma
In angle-closure glaucoma, the iris (the coloured part of the eye) may completely close off the drainage pathway, abruptly blocking the flow of aqueous fluid and leading to a sudden increase in intraocular pressure (IOP). This condition is considered an emergency because optic nerve damage and vision loss can occur within hours of the problem.
Symptoms can include nausea, vomiting, seeing halos around lights and eye pain.
Normal-tension glaucoma
Even some people with “normal” IOP can experience vision loss from glaucoma. This condition is called normal-tension glaucoma.
In this type of glaucoma, the optic nerve is damaged even though the IOP is considered normal. Normal-tension glaucoma is not well understood, but lowering IOP has been shown to slow progression of this form of glaucoma.
Childhood glaucoma
Childhood glaucoma, which starts in infancy, childhood or adolescence, is rare. Like primary open-angle glaucoma, there are few, if any, symptoms in the early stage. Blindness can result if it is left untreated. Like most types of glaucoma, childhood glaucoma may run in families.
Risk Factors
For people with elevated intraocular pressure (IOP), some of the risk factors that will affect whether you will develop glaucoma include:
Your level of IOP
Family history of glaucoma
Your corneal thickness
Certain optic nerve conditions
If you are of a particular ethnic background (African American, East Asian)
Advanced age
If your risk is high, treatment to lower your IOP to prevent future damage is recommended.
Diagnosis
Since glaucoma has no noticeable symptoms, it is a difficult disease to detect without regular, complete eye exams. Ongoing monitoring is needed to watch for changes. During a glaucoma evaluation, you may have the following tests:
Tonometry to test eye pressure
Gonioscopy to determine eye drainage angles
Ophthalmoscopy to assess optic nerve appearance
Visual field test to assess peripheral vision
Optical coherence tomography to assess the thickness of the retina and optic nerve
Tonometry
Tonometry measures your eye pressure by determining how your cornea responds when an instrument (or sometimes a puff of air) presses on the suface of your eye. Eye drops are usually used to numb the surface of your eye for this test.
Gonioscopy
Your eye’s drainage angle is the area where fluid drains out of your eye. During gonioscopy, you sit in a chair facing the microscope used to look inside your eye. You will place your chin on a chin rest and your forehead against a support bar while looking straight ahead.
The goniolens is placed lightly on the front of your eye, and a narrow beam of light is directed into your eye while your doctor looks through the slit lamp at the drainage angle.
Drops will be used to numb the eye before the test.
Ophthalmoscopy
With ophthalmoscopy, a high-powered lens is used to examine the optic nerve and retina.
Sometimes computerized images of the optic nerve are taken to inspect the nerve more closely for damage from elevated pressure in the eye.
Visual field test
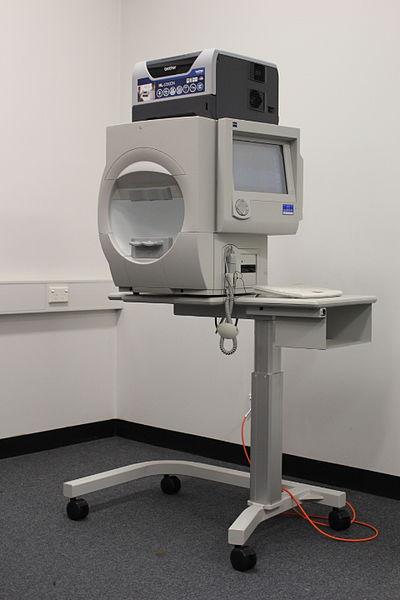
A visual field test can help fi nd certain patterns of vision loss and is a key way to check for glaucoma.
It is very useful in finding early changes in vision caused by nerve damage from glaucoma. This test is done seated at a bowl-shaped instrument called a perimeter. While you stare at the centre of the bowl, lights flash. Each time you see a flash, you press a button. A computer records the location of each fl ash and whether you pressed the button when the light flashed in that location.
At the end of the test, a printout shows if there are areas of your fi eld of vision where you did not see the flashes of light. This test shows if you have any areas of vision loss. Loss of peripheral vision is often an early sign of glaucoma.
Optical coherence tomography (OCT)
A healthy retina (the inner layer of tissue that lines the back of the eye) is only ¼ of a millimetre thick, but it contains multiple layers of specialized cells. One layer converts light into nerve signals, another processes the nerve impulses, while another transmits these processed impulses to the brain where they are interpreted.
Some tests may need to be repeated on a regular basis to monitor any changes in your vision caused by glaucoma.
Treatment
Glaucoma is a chronic disease. While there is no cure for glaucoma, it can often be controlled with proper management.
The goal of glaucoma treatment is to lower your eye pressure to a “target pressure”. This is a level of pressure that is less likely to cause further optic nerve damage. The target pressure differs from individual to individual. Your target pressure may change during your course of treatment.
Medications
You may be prescribed a medication to lower your eye pressure when the risk of vision loss is high enough to justify intervention.
Treatment often consists of eye drops, and there are several different medications available for the treatment of glaucoma. These medications may work by:
1) Decreasing the production of fluid that the eye produces continuously (also known as aqueous humour). The classes of drugs that do this are:
Beta-blockers
Alpha-agonists
Carbonic anhydrase inhibitors
2) Increasing the outflow of the fluid that the eye produces continuously (or aqueous humour). These drugs include prostaglandin analogues.
There may also be combinations of drugs that work together to reduce the production and increase the outflow of aqueous humour.
Laser treatments
Laser treatments may also be used to enhance the drainage of fluid from the eye. They include:
1) Selective laser trabeculoplasty (SLT): A laser procedure to create microscopic bursts of energy in the drainage pathways (the trabecular meshwork) in your eye. These bursts open the drainage holes in the meshwork and allow fluid to drain better through them. This can lower the pressure in your eye and help prevent damage to the optic nerve and loss of vision.
2) Laser peripheral iridotomy: A laser is used to create an opening in the iris (the coloured part of the eye) so that fluid can enter the angle of the eye more easily. It is performed for patients with narrow angles, or angles that look like they might be prone to closure. A special contact lens is put on your eye to help direct the laser’s high-energy beam of light at the iris. The laser makes one or two holes in the iris.
Surgery
For eyes in which drops and laser fail to stop the progression of glaucoma, surgery may be recommended to create a new passage for aqueous fluid to leave the eye. These surgical procedures include:
Trabeculectomy: A procedure where a flap is created in the wall of the eye to allow controlled leakage of fluid into the tissues (conjunctiva) that surround the eye.
Seton: Implanting a drainage reservoir behind the eye and connecting it to the angle drainage structures with a tube that is buried in the eye wall. Fluid then drains to the reservoir, where it is absorbed.
Minimally invasive glaucoma surgery (MIG): This procedure involves inserting tiny devices into the drainage apparatus in the angle to bypass the obstruction and allow the aqueous fluid to drain more readily. There are several devices on the market now, and more are likely to be released in the near future.